
Immunology Cheat Sheet
A guide to the basic biology, clinical development and upcoming readouts in I&I (2023-2024)


Table of contents
Introduction
TYK2
Discovery
Biology
Clinical Development
Future indications and risks
IL-17
Discovery
Biology
Clinical Development
Future indications and risks
IL-23
Discovery
Biology
Clinical Development
Future indications and risks
IL-4/13
Discovery
Biology
Clinical Development
Future indications and risks
TL1A
Discovery
Biology
Clinical Development
Future indications and risks
NLRP3
Discovery
Biology
Clinical Development
Future indications and risks
TSLP
Discovery
Biology
Clinical Development
Future indications and risks
Conclusion
Assets and trials in 2024
Themes in next-gen I&I
Emerging targets
Appendix
Introduction
Calor, rubor, dolor, tumor—it is a mantra that triggers flashbacks to dry pathology lectures in medical school. Yet the impact of these words (heat, redness, pain, swelling) is undeniable.
The “cardinal signs of inflammation,” first described by Celsus in 25 A.D., provide a descriptive framework for disease. As the Romans’ “chief of medicine,” Galen understood this point well—150 years later, he added to Celsus’ work and declared functio laesa (loss of function) to be the “fifth pillar” of inflammation. This was by no means a minor contribution. Linking inflammation to dysfunction is perhaps one of the most important conceptual leaps in medicine.
Celsus and Galen knew not of microbial pathogens, innate or adaptive immunity. However, they recognized that different tissues in the body could undergo similar “cardinal signs” —and that these markers heralded disease.
Modern molecular immunology has vindicated this viewpoint. Activated immune cells that secrete cytokines (e.g. IL-4 IL-6, IL-13, IL-17) to drive skin disorders, also appear to play important roles in joint disease, lung and GI tract pathology. Fundamental immune signaling programs like JAK, TYK2, TL1A, NLRP3 and TSLP are implicated in a growing array of diseases—inhibition of these targets has the potential to benefit many patients.
Understanding the molecular mechanisms that underlie calor, rubor, dolor, tumor and functio laesa is one of the most important areas in biotechnology. In the past couple years, dozens of trials, and billions in government and private funding have been poured into immunology programs. FDA approvals have validated some of these efforts.
What are the most exciting current targets that are “coming of age” in immunology, and how do these molecules drive inflammation and dysfunction? How strong is the clinical evidence to support trials across different indications, and what characteristics will competitive “next-gen” therapies need to possess? For brevity, this “cheat sheet” will focus on assets and programs outside of oncology (where relevant overlaps will be discussed).
Calor, rubor, dolor, tumor, functio laesa. It is hard to imagine Celsus and Galen feeling validated by lucrative M&A deals in the immunology space. Yet they would surely agree that understanding the mechanisms that drive these “cardinal signs” will yield exciting remedies for patients. It is up to the modern scientific, medical and biotech communities to do them justice.
TYK2
Discovery of TYK2
In 1990, a team led by John Krolewski cloned TYK2, which was subsequently found to contain a kinase-like domain with sequence homology to the JAK family of proteins.
Tyk2 deficient mouse models were created in 2000, and utilized to establish a link to IL-10, IL-12 and IL-23 signaling. The first human case of Tyk2 deficiency was reported in 2006, and was implicated in human disease (hyper IgE syndrome).
Several Tyk2 variants have been identified in GWAS studies. “Weak” mutations that only partially dampen signal transduction are protective against psoriasis and systemic lupus erythematosus, whereas stronger loss of function safeguards against ulcerative colitis.
Biology of TYK2
TYK2 promotes type I IFN, IL-6, IL-10, IL-12 and IL-23 signaling and is part of the JAK-STAT pathway.
When a cytokine receptor, such as IL-12R or IFNAR1, binds its ligand, an intracellular subunit (e.g. IL-12RB1) can recruit and phosphorylate TYK2. As part of the JAK-STAT pathway, activated TYK2 can then recruit the transcriptional activator STAT to promote inflammatory responses.
TYK2 modulates downstream signaling from the IL-12, type I interferon, IL-10, IL-4 and IL-13 receptors. Despite binding to the gp130 IL6R subunit, TYK2 does not appear to mediate IL-6 signaling (a cytokine linked to IBD, Castleman’s disease, rheumatoid arthritis and autoimmune disease)

TYK2 Clinical Development
Development of small molecule Tyk2 inhibitors initially focused on targeting the kinase domain. Recent efforts have centered on creating more selective ‘allosteric’ inhibitors that stabilize the pseudokinase domain and “auto-inhibit” the active (kinase) domain of Tyk2.
In 2017, Nimbus Therapeutics published the structure of a bioavailable, selective TYK2 inhibitor (NDI-031301). This academic accomplishment was soon followed by FDA approval of BMS’s deucravacitinib (Sotyktu).
The first FDA approved drug was BMS’s deucravacitinib for treatment of severe plaque psoriasis in late 2022 . “Deucra” targets the pseudokinase domain of Tyk2—theoretically limiting off-target activity inherent molecules targeting the kinase domain.
Traditional JAK inhibitors target the conserved ATP-binding site of the kinase domain, leading to off-target toxicity and a black box warning for the entire JAKi drug class. Decura and selective TYK2i does not carry this warning.

Future indications for Tyk2
Increasingly, companies are looking to exploit TYK2 in novel indications. Biohaven is hoping to use their Tyk2 inhibitor, BHV-200 in the CNS, given its ability to cross the blood brain barrier. Neuron23 has also discussed advancing its own Tyk2 inhibitor for neurologic indications like MS, but clinical trials have not yet been launched.
Mendelian randomisation associations have linked TYK2 loss of function variants with a broad range of indications including hypothyroidism, inflammatory bowel disease, primary biliary cirrhosis and type I diabetes. Diseases which are characterized by the over-expression of type I IFN such as SLE, Sjögren syndrome or systemic sclerosis may benefit from selective Tyk2 inhibition.
There is also some hope that Tyk2 inhibitors may be effective in oncology since activating mutations in the TYK2 gene and over-expression of Tyk2 have been linked to cancer development and progression. The preclinical combination of deucra with MEK blockade decreased proliferation of malignant peripheral nerve sheath tumors.
Several companies including Bristol Myers Squibb, Ventyx, and Oncostellae are pursuing Tyk2 inhibitors in ulcerative colitis. BMS’s deucravacitinib failed to meet its primary endpoint of clinical remission at week 12 or secondary efficacy endpoints in the phase 2 LATTICE-UC study. BMS is still pursuing the drug in UC at a higher dose in their other phase 2 IM011-127 study.
Risks in Tyk2 development
Seucravacitnib which was approved for plaque psoriasis did not achieve PASI 90 or PASI 100 response rates comparable to IL-17 or IL-23, suggesting that TYK2 drugs could be less efficacious in dermatologic indications.
Competition in TYK2 is fierce and capital markets unforgiving: In a Ph2 trial in moderate-severe plaque psoriasis, Ventyx’s VTX958 met its primary endpoint (PASI 75) but did not achieve differentiated efficacy to support future development. The results were released and VTYX dropped almost 70%, despite ongoing trials in IBD (HARMONY) and a robust pipeline including two NLRP3 assets.
A concern with Tyk2i is the occurrence of viral and mycobacterial infections. The most common adverse events noted with deucravacitinib in trials were nasopharyngitis, upper respiratory tract infection, sinusitis, and bronchitis. Pfizer previously halted development of its Tyk2 assets (brepocitinib and PF-06826647) with some speculating that it was due to inadequate efficacy compared to others on the market.
IL-17
Discovery of IL-17
The interleukin-17 family consists of six structurally related cytokines (A-F). Most of the literature focuses on IL-17A, the founding member of the group which was first discovered in 1993 in a rodent T cell library by subtractive hybridization. It was subsequently characterized in humans along with its receptor, IL-17R.
IL-17A was originally cloned and described by Rouvier et al. (1993) It is a disulfide-linked homodimeric glycoprotein with five conserved cysteine residues in the C-termini which form a characteristic knot.
Biology of IL-17
IL-23 is produced by activated dendritic cells and macrophages. In combination with other cytokines, IL-23 induces IL-17 production from Th17 cells by activation of the JAK-STAT cascade and induction of the transcription factor RORγt.
Physiologically, IL-17A is involved in antibacterial and antifungal defense, as it induces the expression of IL-1, TNF and IL-6.
IL-23 inhibition alone is not sufficient to completely suppress IL-17A production, as IL-17 is produced by cells other than Th17.
The IL-17 family of cytokines consists of six structurally similar family members, IL-17A-F, that create distinct homo-/hetero-dimers.While IL-17A is considered to be the most biologically active cytokine in the IL-17 family, IL-17F pathology has been implicated in psoriasis, psoriatic arthritis, hidradenitis suppurativa, and axial spondyloarthritis.

Clinical Development of IL-17 inhibitors
Currently there are four monoclonal anti-IL17 antibodies approved for clinical use: secukinumab and ixekizumab target IL-17A, while bimekizumab targets both IL-17A and IL-17F. Brodalumab inhibits the IL-17 receptor on target tissues, IL-17RA.
The potential of DICE’s oral IL-17 inhibitor compared to the currently improved injectables, Cosentyx and Taltz has not gone unnoticed. In June 2023, Eli Lilly agreed to purchase DICE at a deal price of $48 per share, a total of $2.4 billion in cash.
Moonlake Immunotherapeutics is trialing its anti-IL-17 nanobody sonelokimab in psoriatic arthritis. Across the 207-patient ARGO trial sonelokimab was able to induce a statistically significant response in patients with active psoriatic arthritis compared to placebo: 46% of patients who received the 60-mg dose saw a 50% or greater reduction in signs and symptoms of disease activity. Notably these results were compared to placebo rather than active treatment, such as Humira. When compared directly to Humira (43% response), sonelokimab was not significantly differentiated at the 60mg or 120mg doses -- sending Moonlake stock tumbling 30% upon the data release.
Moonlake is moving forward with phase 3 trials in both hidradenitis suppurativa (HS) and psoriatic arthritis (PsA)—the company hopes that its nanobody format (~40 kDa) will give it an edge over larger mAbs like Bimzelx, Taltz and Cosentyx.
Prior to a negative readout (see below), Acelyrin’s affibody Izokibep was considered exciting due to reduced concerns for immunogenicity and independence from cold chain transportation.
Big miss: Acelyrin’s izokibep recently failed to meet its primary endpoint in its phase 2b/3 trial for HS; despite positive data from MoonLake in the same indication. 39% of patients being treated with izokibep once weekly demonstrated at least a 75% decrease in hidradenitis suppurativa clinical response (HiSCR75) at 16 weeks compared to 29% in the placebo comparator arm (p=0.328). Acelyrin pointed to high rates of discontinuation and an unexpected increase in the placebo response to explain the results — an increasingly common refrain in biotech today.

Future indications for IL-17
In addition to psoriasis, IL-17 inhibitors have mostly been trialed in PsA and HS, with Ph2 trials from Acelyrin and Moonlake providing underwhelming data to date. IL-17 inhibition is also being examined in axial spondyloarthritis in a Ph3 trial by UCB.
In Phase 2 PsA studies, Moonlake’s sonelkinumab did not outperform Humira; in an earlier HS study the company did not disclose a direct Humira comparison (nor results from a higher dose sonelkinumab cohort) — raising doubts about the selectivity and differentiation of this drug class in these indications. Cosentyx also gained approval for HS in October 2023—adding another layer of competition for smaller companies like Moonlake and Acelyrin.
There is increasing focus on the role of IL-17 in other conditions including Behcet’s syndrome, where elevated levels of this cytokine are associated with skin and mucus lesions and the development of uveitis.
The IL-17/IL-23 axis has also been identified as important in other eye disorders including sympathetic ophthalmia, eye lesions from sarcoidosis, and chorioretinitis. Other promising areas include respiratory disease such as asthma, cystic fibrosis, and COPD.
Risks in IL-17 development
Several factors challenge the potential of IL-17 inhibitors. Firstly they increase the risk of fungal and upper respiratory tract bacterial infection. Bimekizumab which neutralizes IL-17A and IL-17F is associated with a higher incidence of oral candidiasis than secukinumab, which solely neutralizes IL-17A.
A meta-analysis evaluated the incidence of adverse effects in patients treated with IL-17 inhibitors and found that with treatments lasting more than one year, the incidence of adverse events could be as high as 72.0%, and long-term use could predispose to psychiatric disease. A phase III trial involving brodalumab was stopped because six participants developed suicidal behavior (though the true nature of these events are currently not known).
IL-17 inhibitors carry a risk of immunogenicity leading to the development of anti-drug antibodies, which can affect pharmacokinetic, pharmacodynamics and bioavailability. The risk of immunogenicity varies depending on the antibody used: brodalumab (2.7%), ixekizumab (9%), and secukinumab (0.41%).
IL-23
Discovery of IL-23
IL-23 was identified in 2000 as part of an in silico search for novel members of the IL-6 cytokine family. It is a heterodimeric cytokine consisting of p40 (identical to IL-12 subunit) and p19. Due to a shared p40 subunit, much of the pathophysiology previously ascribed to IL-12 (between 1989 and 2002) was driven by IL-23.
In 2003, Daniel Cua recognised that IL-23 was a key player in autoimmune inflammation by examining the relative contribution of IL-12 and IL-23 using deficient mice.
Biology of IL-23
IL-23 is produced by activated macrophages and dendritic cells and acts on the IL-23 receptor which is expressed on a variety of cells including T cells, innate lymphoid cells, intraepithelial lymphocytes and NK cells.
IL-23R signals through the JAK-STAT pathway resulting in pro-inflammatory cytokine production. In the absence of IL-23, Th17 cells transform to Treg FOXP3+ which cannot produce IL-17.
IL-23 plays an important role in antigen-mediated T cell responses and in seronegative diseases. It is important at the body’s external barrier surfaces such as the skin and gut and in high biomechanical stress tissues such as the joints.

Clinical development of IL-23 mAbs
There are currently 4 FDA approved IL-23 inhibitors: ildrakizumab-asmn (marketed as Ilumya) was developed by Sun Pharmaceuticals and approved for treatment of plaque psoriasis based the SURFACE1 and reSURFACE 2 Ph3 trials.
Ustekinumab (Stelara) was developed by Janssen Biotech (part of Johnson and Johnson) and is approved for plaque psoriasis, psoriatic arthritis, Crohn’s disease and ulcerative colitis. Janssen Biotech also developed Guselkumab (Tremfya) which is FDA approved to treat plaque psoriasis and psoriatic arthritis.

Future and risks in IL-23 development
IL-23 agents are being explored for use in psoriasis and inflammatory bowel disease. However early data suggests that these drugs may also have benefits in rheumatoid arthritis and multiple sclerosis.
There is some concern that IL-23 inhibitors may not be as efficacious as other assets: AstraZeneca discontinued further exploration of brazikumab following its phase 2a trials in June 2023.
There is increasing focus on identifying possible predictors of response to create a tailored approach to therapy. If testing for TNFR2+IL23R+ T cells and tissue IL-22 levels before initiation of therapy becomes readily available this would make the decision between starting an anti-TNF or IL-23 inhibitor much clearer, improving the ease of use in clinical practice.
Overall, the safety profile of anti-IL-23 agents appears favorable. There does not seem to be a clear infection risk or evidence of neoplastic or cardiovascular complications in previous trials extending to 33 months.
IL-4 and IL-13
Discovery of IL-4/13
IL-4 was discovered in the early 1980s by Maureen Howard and William E. Paul. They were studying induction of B-cell proliferation by anti-IgM antibodies and noticed a correlation with cell density. They tested the supernatant and found a factor that accelerated B-cell growth, which they named B cell growth factor (BCGF).
After being molecularly cloned this factor was renamed as “IL-4.” In 1986, the Paul and Bob Coffman labs demonstrated the role of IL-4 as a T cell and mast cell growth factor.
IL-13 was first discovered in the laboratory of Dr. Mossman in 1989, as a close congener of IL-4. IL-13 can mediate virtually all of IL-4 actions on non-hematopoietic cells and to some degree on hematopoietic cells.
Il4 and il13 are very close to one another on chromosome 5, are often co-expressed, and share receptor components and biological activities.
Biology of IL-4/13
IL-4 binds to IL-4Rα which is widely expressed. This leads to generation of a ligand receptor complex that involves recruitment of a third receptor chain either IL-2Rγc (γc) or IL-13Rα1. The complex formed with γc is a type I IL-4 receptor and whereas IL-13Rα1 is a type II IL-4 receptor.
IL-13 has two receptors and utilizes two separate binding chains, IL-13Rα1 and IL-13Rα2. IL-13Rα2 binds IL-13 with higher affinity than IL-13Rα1. IL-13Rα2 is considered to be a decoy receptor that “neutralizes” IL-13. When IL-13 binds IL-13Rα1, IL-4Rα is recruited into the receptor complex which then activates STAT6.
IL-4 drives Th2 differentiation, class switching for immunoglobulins and production of other cytokines like IL-12. IL-13 has more effector cytokine functions in allergic responses (e.g. asthma), and regulates smooth muscle contraction and mucus production in the airway as an example.

Clinical development of IL-4 and IL-13

Future indications and risks in IL-4 and IL-13 development
Dupilumab, which blocks both IL-4 and IL-13 via IL-4Rα antagonism, is currently FDA approved for asthma, chronic rhino-sinusitis, moderate to severe atopic dermatitis, prurigo nodularis, and eosinophilic esophagitis.
Whether these changes are durable in real world patients remains to be seen— longterm post-marketing efforts like RAPID (following asthma patients on dupixent), are critical to document the full impact of this drug on patients with airway disease.
Targeting IL-13 (which has a longer half-life than IL-4R), may lead to more convenient dosing regimes compared to drugs like dupilumab (dosed q2 weeks). Trials of Eli Lilly’s lebrikizumab (in AD) and Apogee’s earlier stage IL-13 asset will be interesting to watch with respect to this point (dosing every 1-2 months).
In phase III trials for COPD, dupilumab scored a big win, meeting all primary and secondary endpoints. The primary endpoint was the annualized rate of moderate or severe exacerbations of COPD. This was 0.78 (95% CI, 0.64 to 0.93) with dupilumab and 1.10 (95% CI, 0.93 to 1.30) with placebo (rate ratio, 0.70; 95% CI, 0.58 to 0.86; P<0.001).
There do not seem to be any glaring safety concerns or toxicity attributed to IL-4/IL-13 inhibitors. A systematic review identified an expected impairment in the helminth infection response but did not observe any other safety risks relating to infection, malignancy or cardiovascular events.
TL1A
Discovery of TL1A
DR3, TL1A’s receptor was cloned in the mid 1990s by a number of groups as a TNF-family receptor with high homology to TNFR1. It was noted to be primarily expressed in lymphocytes and mediates inflammatory responses.
TL1A is a tumor necrosis factor family member that is expressed by dendritic cells, monocytes, macrophages, fibroblasts and endothelial cells. It was first discovered in 2002 and has roles in the innate and adaptive immune systems.
Soluble TL1A (sTL1A) has been detected in the serum of patients with T-cell mediated autoimmune diseases such as rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis.
Biology of TL1A
TL1A binds to DR3, a cell surface receptor that is mostly expressed on T cells. In various experimental systems, the binding of TL1A to DR3 has the downstream effect of amplifying all major T cell effector responses including Th1, Th2, Th9, and Th17.
The first in vivo evidence of the role of TL1A in IBD came from two independent research groups that developed transgenic mice to over-express TL1A. The effects included increased IL-13 the small intestine and intestinal inflammation localized to the ileum.
Human evidence came from several genome wide association studies in inflammatory bowel disease. There are 3 haplotypes for TNFSF15 that confer either increased risk or protection from developing IBD. Characterization of the mucosal expression profiles demonstrated increased expression of TL1A and DR3 in areas of active inflammation in IBD patients.

Clinical development of TL1A inhibitors
Future development and risks in TL1A
TL1A is upregulated in intestinal, joint and skin tissues, and has been detected in the serum of patients with psoriasis, primary biliary cirrhosis, SLE and ankylosing spondylitis. Experiments in lesions of psoriasis mouse models showed that treatment with anti-TL1A antibody reduced histopathological changes and IL-17 levels.
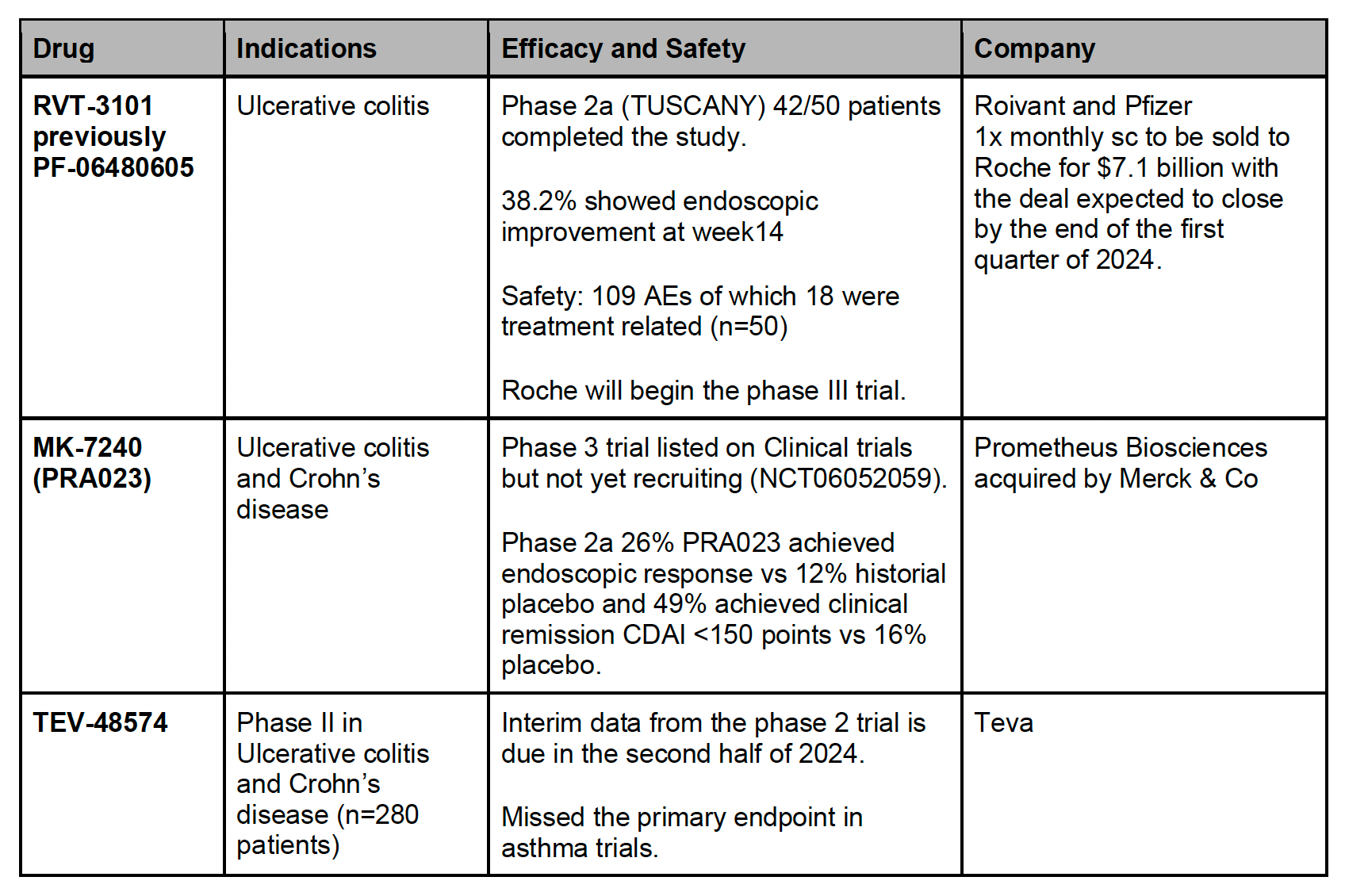
It is important to note that TL1A/DR3 signaling lacks specificity and may act in both pro- and anti-inflammatory ways. In the phase 2 trial of RVT-3101 (TUSCANY-2 trial), the most common adverse event was (paradoxically) an exacerbation of ulcerative colitis.
Clinical concerns about TL1A inhibitors included the inconvenient requirement for multiple iv infusions and the high immunogenicity rates. For example, in the TUSCANY study for RVT-3101, 41 participants tested positive for anti-drug antibodies and 5 (10%) for neutralizing antibodies.
NLRP3
Discovery of NLRP3
The NOD-like receptor (NLR) family pyrin domain containing protein 3 (NLRP3) is a pattern recognition receptor (PRR) which responds to a wide range of stimuli including LPS, ATP, high fat and high sugar diet.
The human NLR family is characterized by a tripartite structure:
Central domain that mediates nucleotide binding and oligomerization referred to as a NACHT domain
C-terminal LRR domain that senses NLR agonists but is auto-inhibitory in their absence
Variable N-terminal domain required for homotypic protein-protein interactions
The inflammasome was first described in 2002 by Dr. Jurg Tschopp and colleagues as an inflammatory ‘caspase activating complex’. Two years later, the same group discovered NLRP3 by looking at macrophages from those with Muckle-Wells syndrome (MWS).
In 2004, Tschopp and colleagues demonstrated that NLRP3 inflammasome-dependent disorders are due to spontaneous, excessive production of IL-1β.
Biology of NLRP3
The inflammasome is tightly regulated and involves a two-step process: priming and then activation. “Priming” upregulates the expression of inflammasome components and also induces post-translational modifications of NLRP3 to create a signal-competent state.
There are a broad range of activating signals including LPS, extracellular ATP, ion flux and production of ROS which can induce NLRP3 assembly and inflammatory caspase activation. Caspase-1/11 can the process IL-1 family cytokines and allow for their secretion.
A variety of NLRP3 inhibitors have shown promising efficacy in animal models of inflammatory diseases—namely MCC905, an NLRP3-specific small molecule inhibitor.

Clinical development of NLRP3 inhibitors
Future development and risks in NLRP3
The first generation of NLRP3 inhibitors had several limitations. Poor pharmacodynamics and pharmacokinetics of MCC950 has limited its clinical applications to date. Another small molecule inhibitor, known as BHB, was shown to inhibit NLRP3 inflammasome activation and had an anti-inflammatory role in the animal models of Alzheimer’s Disease and gout, but had poor therapeutic effect in acute inflammatory diseases.
Preclinical data involving genetically modified mouse models has stimulated a research interest in cardiovascular disease. Colchicine is a non-selective NLRP3 inhibitor that has shown to be effective in pericarditis and risk reduction in coronary artery disease. There are several targeted inflammasome inhibitors under development but the clinical data is currently insufficient.
TSLP
Discovery of TSLP
TSLP was first identified in mice as a secreted factor from thymic stromal cells. In vitro, TSLP stimulated thymocyte and B cell lymphopoiesis. The human homolog was discovered in an effort (Kastelein and Bazan) to identify new members of the IL-17 family of cytokines. TSLP was originally labeled as IL-50 and was structurally dissimilar from murine TSLP.
Vassili Soumelis and Yong-Jun Liu at the DNAX Research Institute worked to functionally characterize human TSLP. They found that TSLP was a strong inducer of Th2 cytokines and TNF. In vitro cellular screens found that activated epithelial cells (bronchial and alveolar in particular) were an important source of TSLP.
In 2000, several groups identified a receptor that could bind TSLP. TSLPR is a heterodimeric receptor consisting of the TSLPR subunit and IL-7Rα subunit; it is expressed by several haematopoietic cell populations such as T cells, DCs and non-haematopoietic cells such as epithelial cells.
Biology of TSLP
TSLP is a key factor in maintaining immune homeostasis and regulating inflammatory responses at the mucosal barrier. It is a distant paralog of IL-17. It is an epithelium derived cytokine and is an important driver of type 2 inflammatory diseases including atopic dermatitis, food hypersensitivity, and asthma. Collectively, molecules like TSLP, IL-33 and IL-25 are referred to as ‘alarmins’.
TSLP is a member of the hematopoietin receptor family and was found to activate JAK-1 and JAK-2 followed by STAT 1,3,4,5 and 6 depending on the cell type.
TSLP is an important driver of atopic dermatitis with both acute and chronic AD lesions showing high levels of TSLP expression in differentiated keratinocytes.
In asthma, genome-wide association studies demonstrated that the TSLP SNP rs1837253 was significantly associated with asthma risk in three ethnic groups. Biopsies in patients with severe asthmatic disease showed increased expression of TSLP in the airway epithelium and lamina propria. Tezepelumab significantly reduced blood and sputum eosinophils and exhaled nitric oxide and significantly reduced both early-phase and late-phase allergen-induced bronchoconstriction.

Clinical development of TSLP inhibitors
Ecleralimab (developed by Novartis) recently posted results of its placebo-controlled trial in mild asthma (n=28). The primary end-points were the allergen-induced change in FEV1 during the late asthmatic response (LAR) measured by area under the curve (AUC3-7h) and maximum percentage decrease (LAR%) on day 84 as compared to placebo.
On day 84, patients receiving ecleralimab had significantly attenuated LAR AUC3–7h: 4.2% in the ecleralimab group (n=15) and 11.38% in the placebo (n=13), representing a 64% reduction (p=0.008)
Ecleralimab patients also exhibited a 64% decrease in sputum eosinophils at 7 h (p=0.011) and a 52% decrease at 24 h (p=0.047), following challenge with allergen.
Aiolos recently announced a $245M series A funding to run definitive trials for their TSLP asset in airway disease. AIO-001 is in-licensed from a Chinese biotech company Jiangsu Hengrui Pharmaceuticals Co—Aiolos has global development and commercialization rights outside of China.
Upstream Bio raised $200 million in a series B to help advance UPB-001 (currently Ph1b for asthma) into phase II trials for asthma and chronic rhinosinusitis with nasal polyps.
UPB-001 is a fully human IgG1 mAb targeting the TSLP receptor and pre clinical data showed a 5-fold increased potency compared to TSLP ligand. TRAEs were reported in 21/42 in the UPB-001 group and 3/14 in the placebo group. The most common were headache and dysmenorrhoea.

Future development and risks in TSLP
TSLP has been implicated in the induction and progression of several tumors including solid and hematological tumors. TSLP is secreted by cancer-associated fibroblasts or tumor cells to promote a Th2 tumor microenvironment which leads to worse prognosis in pancreatic cancer, breast cancer and gastric cancer. A range of studies indicated that TSLP inhibition can be beneficial or deleterious, depending on the malignancy and biological context. More work is needed to explore the clinical indications where blocking or augmenting TSLP would be appropriate.
Conclusion: the future of I&I
Assets and trials to watch in 2024
TL1A is one of the most exciting targets in IBD, and has attracted a lot of strategic interest in 2023. However, the TL1A space has quickly gotten crowded, and companies like Teva are trailing Merck and Telavant. We don't know how to gauge a “best in class” TL1A inhibitor, as Ph3 data is still forthcoming—but ~25% placebo adjusted clinical remission is the bar to beat in UC. Aeglea/Spyre is also tossing its hat in the ring for a “best in class” TL1A, with FiH studies slated to begin in 2H24.
The TYK2 space has had its ups and downs in 2023. The recent underwhelming results for Ventyx in psoriasis has tempered expectations for future studies. In psoriasis, VTX958 was unable to clear the bar set by deucravacitinib and Takeda's TAK-279, despite achieving target IC90 exposure levels. Therefore, whether these target exposures will translate into efficacy for indications like Crohn's disease (topline readout 2024) is in question. Ventyx also had high discontinuation rates and dosed much higher than deucra and TAK-279 - something to watch in future trials. Deucra’s (Sotyktu) impending patent expiration in 2033 may drive shifts in the reimbursement landscape, making it difficult for late entrants targeting TYK2 to compete.
Half-life extension and “me-betters”: Groups like Apogee, Spyre, Viridian and Aiolos are developing half-life extended biologics in chronic disease areas where convenience (less frequent dosing) may be a driver of clinical uptake. For these assets, the biology is well-validated, and risks depend on execution of late stage studies and commercialization: what level of optimization actually moves the needle for payers and patients?

Themes for next-gen assets
Precision immunology: Biomarkers that allow for patient stratification will usher in the age of “precision immunology.” Autoimmune disease is multifactorial and heterogeneous, making it difficult to find robust markers of disease onset, progression and response to therapy. Yet we have seen some intriguing early efforts with Prometheus’s companion diagnostic for their anti-TL1A in UC. Other companies pursuing companion diagnostics for their I&I assets include Neuron23 (LRRK2&TYK2) and Aeglea/Spyre (undisclosed CDx).
Head-to-head comparisons with standard of care agents in clinical trials
Given the complexity of the treatment landscape in autoimmune disease, demonstration of efficacy over standard of care is key (see the above discussion about Moonlake’s PsA trials for its anti-IL-17).
Despite the availability of several treatment options in diseases like RA and UC, clinical efficacy attained by existing agents leaves a lot to be desired, creating ‘white space’ for new mechanisms of action or improved drug profiles for known targets. In other spaces like psoriasis, the bar is quite high: delivering meaningful efficacy over approved agents like Cosentyx may prove challenging.
Companies with oral analogs for validated targets will be exciting to watch. The key question is around target coverage - using a small molecule, can one achieve the same degree of inhibition as an antibody?
Dice/Lilly (IL-17; NCT05896527), Protagonist/Janssen (IL-23; NCT06095102/NCT06095115), Sanofi (TNF; NCT06073093/NCT06073119) are some key programs to watch in 2024-1H25. Morphic is developing an “oral Entyvio” that inhibits the a4b7 integrin for use in ulcerative colitis—though recent data from Morphic suggests lower rates of endoscopic improvement than its approved mAb counterpart from Takeda (full Ph2b trial data can be expected from MORF in 2025).
Novel indications: patient need should drive indication selection.
Outside of corticosteroid therapy, there are few treatments for advanced COPD. Dupixent’s stellar results in phase III trials NOTUS and BOREAS included a 34% reduction in exacerbations compared to placebo, and opens up this space for other assets in I&I.
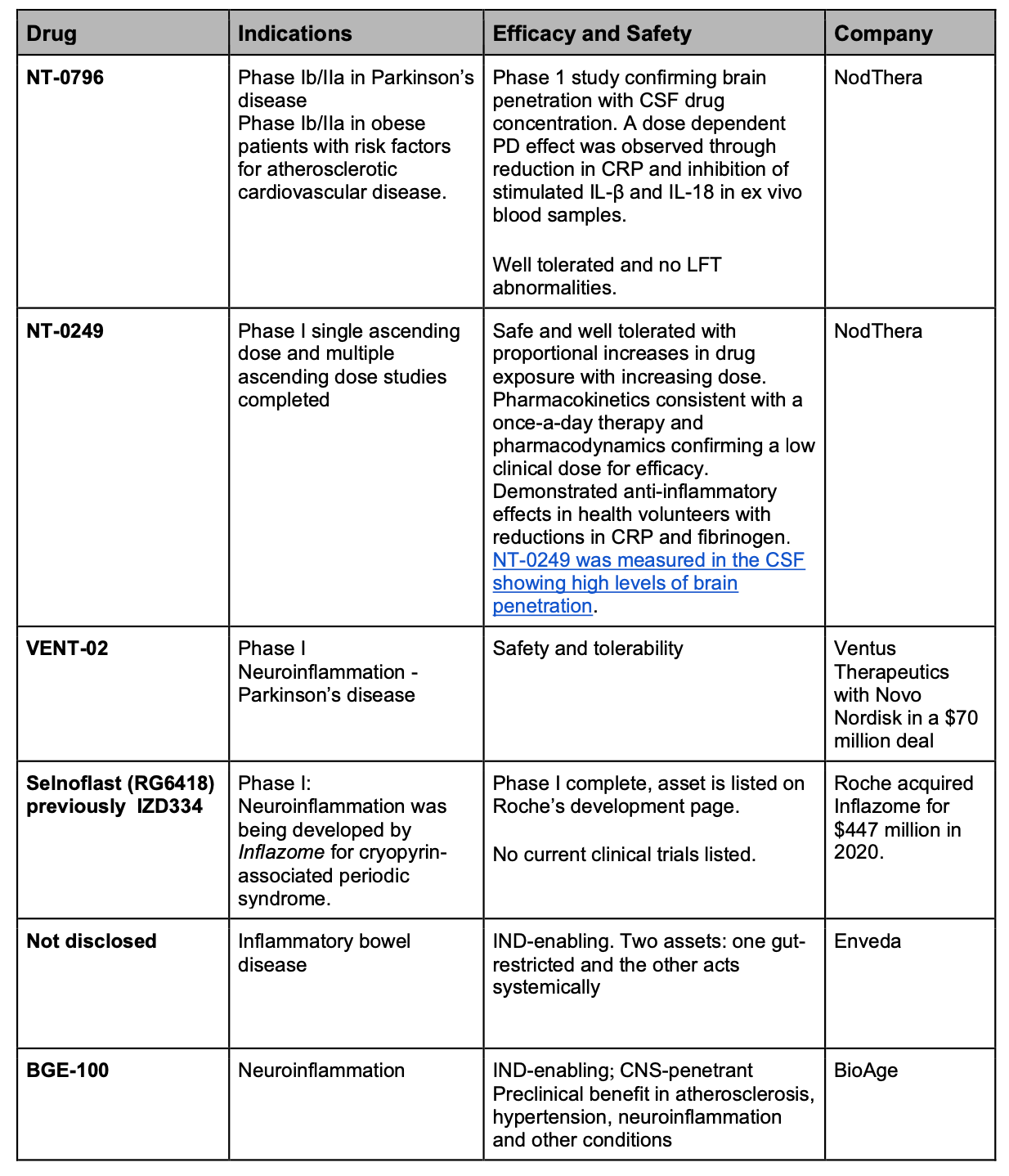
Application of the discussed agents to dampen neuroinflammation may prove useful in neurodegenerative disease. Neuron23 is developing a peripherally restricted TYK2 inhibitor for IBD, and a brain-penetrant asset for MS. With their FcRn antagonist approaches, companies like Argenx, Immunovant, UCB and Biohaven are taking on a wide number of immunologic indications with high unmet need: bullous pemphigoid, Sjogren’s, and inflammatory myopathies to name a few. Given the role of autoantibodies in these conditions, cell therapies targeting B cells may also be well-positioned to address some of these pathologies.
Cell therapies and other emerging (and old) modalities: despite the strides made in the autoimmune space over the last several years, many diseases remain underserved by current approaches. Many now seek to exploit established oncology modalities (cell and immunotherapy) in I&I.
CAR-Ts may be widely applicable in autoimmune diseases, especially where B cells may be key drivers. Paired with a lymphodepletion protocol, CAR-T therapy may offer an opportunity for a “B cell reset.” Autologous cell therapies are being explored in several disease areas outside of SLE, including systemic sclerosis, MS, MG, PV, myositis, ITP, T1D. CRISPR Therapeutics recently announced their plans to expand into autoimmune disease.
If approved, CAR-Ts will likely be used in more severe, refractory patients, but the ultimate addressable patient population remains contested. In the next 12-24 months, we may have a view of early differentiation emerging between programs (table below for SLE).
The FDA recently submitted an official statement on an investigation into T-cell malignancies following BCMA- or CD19-directed autologous CAR-T cell therapies, which may impact companies developing CAR-Ts for I&I.
Other modalities in development:
Degraders: Oncology targeted protein degrader companies like Kymera and Monte Rosa are now setting their sights on autoimmune disease. Early stage extracellular degradation companies like Avilar, EpiBiologics and Lycia may seek to leverage their platforms to target IgG or pro-inflammatory cytokines.
Checkpoint modulation: Anaptys Bio is developing a PD-1 agonist for RA and UC, as well as a BTLA agonist for AD. Gilead acquired Miro Bio last year for $405M for its portfolio of checkpoint agonists.
Targeted immunosuppression: AbbVie was developing an antibody-drug conjugate in which a steroid was linked to Humira, but was discontinued due to “Changes in biomarkers consistent with systemic steroid exposure.” Tarepyo recently gained approval for IgAN by targeting mucosal (Peyer’s patch) B cells with potent corticosterioid—suppressing production of IgA and sparing tissues from systemic steroid exposure.

Emerging targets in immunology
IRAK4: TLRs and IL-1Rs are implicated in the pathogenesis of hidradenitis suppurativa and atopic dermatitis and signal through the myddosome. IL-1 receptor-associated kinase 4 (IRAK4) is essential for assembly of the myddosome and activation of NF--κB and MAP kinases.
Kymera/Sanofi are developing a IRAK4 degrader for atopic derm (Ph2).
STAT6: The IL-4R-STAT6 axis is involved in type-2 immunity, and dysregulation of STAT6 signaling drives a pathogenic role in Th2 cell-mediated allergic disease. Human gain-of-function STAT6 variants have been identified in the pathogenesis or exacerbation of multiple allergic diseases, including asthma, food allergy, and atopic dermatitis.
Sanofi inked a deal worth $1.3B with Recludix Pharma this year for the development and commercialization of STAT6 small molecule inhibitors.
MRGPRX2: The Mas-related GPR family member X2 (MRGPRX2) GPCR was recently identified as a prominent driver of IgE-independent degranulation of mast cells, provoking allergic inflammatory reactions. Functional analyses of urticaria patient mast cells and assessment of skin samples from atopic dermatitis patients suggest a pathophysiologic contribution of the receptor to these conditions.
Escient Pharmaceuticals is examining EP262, a small molecule antagonist of MRGPRX2, in Ph1b/2 trials for chronic inducible urticaria, chronic spontaneous urticaria, and atopic dermatitis.
FcRn: IgG-mediated autoimmune diseases include myasthenia gravis, IBD, RA and multiple sclerosis. The role of the neonatal Fc receptor (FcRn) in these disorders was recognized in the 1990s through the use of knockout B2m−/− mice, showing the necessity of FcRn to a disease phenotype. Several therapeutics to prevent FcRn–IgG interactions have been developed.
Argenx’s efgartigimod has been approved for myasthenia gravis, and is in trials for over 15 indications across autoimmune disease. The drug recently failed to meet its endpoint in immune thrombocytopenia (ITP), causing some concern about pipeline in product potential.
Roivant (immunovant) is also developing an FcRn mAb that is being pursued in a broad range of indications, including a Ph2b trial in CIDP with a readout expected in 2024.
Biohaven is attempting to develop a novel approach through its bispecific IgG degrader, BHV-1300. The molecule will interact with Hepatic asialoglycoprotein receptor (ASGPR) to target pathogenic isoforms of IgG. Hopefully, this novel approach will not cause dyslipidemia or hypoalbuminaemia that has been linked to FcRn inhibitors.
APRIL: member of the TNF superfamily of cytokines and has a physiological role in the regulation of B-cell mediated immune responses. It acts through 2 different receptors: TACI and BCMA. APRIL interacting with TACI mediated IgA class switch recombination. Blocking APRIL may help reduce circulating levels of both total IgA and aberrantly glycosylated IgA.
GWAS demonstrated TNFSF13 (the gene encoding APRIL) as a risk locus for IgAN. In a study of 410 patients, those who had the highest APRIL plasma levels had a greater than 10-fold risk of kidney failure, with adjustment for baseline covariates.
Several studies evaluating APRIL inhibition in IgA nephropathy are underway: Chinook (acquired by Novartis) is developing a humanized IgG4 anti-APRIL mAb and is currently enrolling in phase 3 BEYOND IgAN trials.
Appendix
 | A guest post by
|
Competition in the TYK2 drug market is intensifying, and Pfizer will sell 2 drugs under development
https://worldwidechemicallabs.us/
Competition in the TYK2 drug market is intensifying, and Pfizer will sell 2 drugs under development
https://worldwidechemicallabs.us/